Cryopreservation of Large Number of Human Hematopoietic Cells – A Model for Research Space with Limited Resources
Seda Ayer, Steven J. Greco, Khadidiatou Guiro, Lauren S. Sherman, Bobak Shadpoor, Andrew Petryna, Yannick Kenfack and Pranela Rameshwar*
Department of Medicine, Rutgers School of Medicine, Newark, NJ, USA
E-mail: rameshwa@njms.rutgers.edu
*Corresponding Author
Received 19 May 2023; Accepted 22 July 2023; Publication 03 February 2024
Unlike cell lines, cells from primary human tissues are valuable, requiring storage for long-term use. Large number of primary cells require the most efficient method of shipment, when relevant, and cryopreservation to preserve the viability and function. Shipping of cells could be determined by the specific experimental question. These issues are particularly important for primary cells such as hematopoietic stem cells, which cannot expand in vitro. There is minimum issues when cryopreserving relatively small number of cells from tissues such as umbilical cord blood and bone marrow aspirates. However, cryopreservation of 200 10 primary cells comes with challenges to identify the most efficient method for long-term storage. Here we report on processes to achieve efficient cell health and recovery of hematopoietic cells from mobilized peripheral blood cells (MPBs). We also determined overnight shipment of MPBs led to overall outcomes when shipped in the cold, as compared to room temperature. We found that cryopreservation of 50 10 cells in 2 mL led to maximum recovery of hematopoietic cell subsets. The implication for these conditions to achieve efficient long-term storage is discussed. These methods will benefit small research laboratories such as those at academic settings and start-up companies with limited resources.
Keywords: Cell storage, cryopreservation, mobilized peripheral blood, transplant, stem cell, hematopoiesis.
Cell therapy, which includes stem cells for solid and hematological cancers, as well as the use of stem cells and/or their secretome in the area of regenerative medicine, are morphing as standard clinical practice [1–3]. To effectively translate cellular products to patients, it is imperative to conduct basic and clinical research. In general, these research studies are conducted in small operational laboratories, mostly in academic settings. Similar research studies are also conducted in biotechnology companies. In many instances, these laboratories rely on clinical collaboration to acquire human cells from tissues such as blood, adipose tissue, placenta, bone marrow and/or mobilized peripheral blood (MPB). This requires that the laboratories build a bank of cells for ongoing and subsequent research. More importantly, scientists are required to ensure that their donor pools represent all ethnic backgrounds. This is important because it is crucial to ensure that the research can be applied to all ethnic groups. If not, the research could lead to costly failure of the research as it gets to the clinical phase.
Although cryopreserving small numbers of cells is routine, recovery of viable cells when storing large numbers per vial is less reliable. The stance for storing large number of cells per vial is mainly due to limited space, resources, and the need to preserve cells for long-term studies. Therefore, the goal for any laboratory is to develop a method that cryopreserves a large number of cells that, when thawed, should have excellent viability and retain cell function.
In general, cryopreservation of cell lines such as those from tumors can be easily established since most cell lines can expand through multiple passages without loss of function. In these cases, the laboratory can cryopreserve a small number of cells in relatively few vials. These vials can be replaced with continued expansion of the cell lines. However, there are challenges when handling primary healthy cells, mostly due to the inability to expand primary cells in culture without transitioning them to cell lines. Thus, it is important to optimize a cryopreservation method that is efficient with respect to viability and recovered functions. Here we describe a method to cryopreserve a relatively large number of primary human/hematopoietic cells.
We report on an optimized method to cryopreserve MPBs. MBPs are acquired after a donor is given granulocyte colony stimulating factor (G-CSF) or other similar mobilizing agents to get hematopoietic stem and progenitors into the peripheral blood [4]. This method has mostly replaced the invasive procedure with bone marrow aspiration to harvest similar hematopoietic cells [5]. We conducted exhaustive research using varied parameters to achieve sustained cell viability and function with the cryopreserved cells [6]. We showed an efficient method that eliminates cell death while preserving the phenotype.
Powdered Human Serum Albumin (HSA) was purchased from Irvine Scientific (Santa Ana, CA); liquid HSA from Irvine Scientific (Santa Ana, CA); dimethyl sulfoxide (DMSO), RPMI 1640, tissue culture grade phosphate buffered saline (PBS) and USP graded normal saline from ThermoFisher Scientific (Waltham, MA), waterless ice bucket from Cole-Parmer (Vernon Hills, IL), LIVE/DEAD cell vitality assay kit from ThermoFisher Scientific, CryoStor Freeze solution and Hypothermosol from Hemacare (Northridge, LA, CA); and 7-amino-actinomycin D from Life Technology (Carlsbad, CA).
The following antibodies were purchased from BD Biosciences (San Jose, CA): PerCP-Cy5.5 murine anti-human CD45, FITC murine anti-human CD45, APC murine anti-human CD34, PE murine anti-human CD38, PE murine anti-human CD33, PE murine anti-human CD56, PE murine anti-human CD19, APC murine anti-human CD3; PerCP-Cy5.5 Mouse IgG1 Isotype Control, APC Mouse IgG1 Isotype Control, PE Mouse IgG1 Isotype Control, and FITC Mouse IgG1 Isotype Control.
The method to acquire MPB has been described [6]. MPBs were obtained from HemaCare (Northridge, LA, CA). The collection of MPBs and demographics of donors were previously described [6]. The collection of MPBs followed an approved protocol by Rutgers Institutional Review Board, NJ. The MPBs were shipped on ice (4C) or at room temperature (25C) in 200 mL volume of Leukopak.
The method to select CD34 cells was previously described [6]. Briefly, we selected CD34 cells with CD34 microbead human kit (Miltenyi, Auburn, CA, USA) as per manufacturer’s instructions. Total nucleated cells from the shipped MPBs were centrifuged and then resuspended in cold MACS buffer at 10 cells/300 L buffer. The cell suspension was incubated in 100 L of FcR Blocking Reagent and CD34 MicroBeads and then incubated for 30 min on ice. This was followed by a cell wash using the MACS buffer. The washed cells were used to positively select CD34 cells with a magnetic separation.
Leukopak cells were cryopreserved with freshly prepared 4.5% HSA containing 20% DMSO. Lyophilized HSA was reconstituted in normal saline, and liquid HSA diluted in saline. The solutions were filtered through 0.2 membranes and then equilibrated at 4C for greater than 10 mins before adding to the cells. Cryostor cryopreservation media contained 20% DMSO.
The leukopak containing the MPB cells was maintained cold in a standing position. This was achieved by anchoring the cells between two icepacks and, in some cases, carefully placing the bag in an upright position in a waterless ice bucket. Since the total volume of MPBs was 200 mL, we dropwise added 200 mL of the cryopreservation media while gently shaking the bag. This resulted in 50 10 nucleated cells/vial. The cell solution was aliquoted in 2 mL vials. The vials were immediately transferred to a controlled rate freezer (Cryo Met Freezer, ThermoFisher) at 1C/min. The cells were removed when the temperature reached 100C to liquid nitrogen.
Optimization also required us to double or quadruple the total number of cells in the cryovials. This required removing centrifuging the solution to remove the appropriate amount of leukopak then to continue as above. The methods were compared with Hypothermosol, which required short term storage of the cells in the cold, and with the commercial freezing media, Cyostor.
Cells (10) were incubated with the primary antibodies in 100 l PBS. Background labeling was assessed by parallel incubation with isotype IgG using the same concentration as the primary antibodies. After 30 mins at room temperature, the cells were washed with PBS and then immediately acquired on a FACSCalibur flow cytometer (BD Biosciences). The data were analyzed using BD CellQuest Pro software (BD Biosciences).
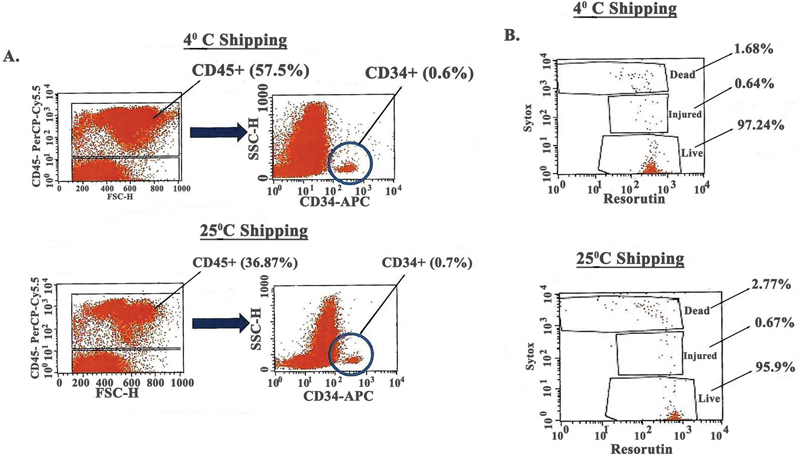
We performed flow cytometry to identify the percentages of CD34 cells in shipped MPBs. The MPBs from the same donor were shipped in aliquots of 90 mL at 4C or at room temperature (25C). The approximate time during shipment was 16 h. The shipped cells were co-labeled with anti-CD34 and -CD45 and then analyzed on the FACScan (BD Biosciences). There was 57.5% total CD45 cells within cells shipped at 4C, and 36.87% at 25C shipment (Figure 1A). We expected a higher percentage of CD45 cells, suggesting that there could be dim expression that could not detect all of the CD45. Since endothelial cells are CD34, their incorporation in the analyses was determined by gating the CD45 cells, which allowed for the analyses of only hematopoietic cells. After this, we gated the CD34 cells. The results indicated 0.6% and 0.7% CD34 cells at 4C and 25C shipment, respectively (Figure 1A). Although the data suggested dim the CD45 cells, the percentages of CD34 cells are in line with the literature [7]. Thus, it is possible that cells within the CD45 dim population were in the mature immune cells.
Figure 1 Post-shipped characterization of MPBs. A) Flow cytometry to determine the percentage of CD34 cells within the CD45 subset in samples shipped at 4C and 25C. B) Vitality assay for health of cells.
We studied cell health at each shipment condition using the LIVE/DEAD cell vitality assay kit. There were similar percentages of dead, injured, and live cells in both shipping methods (Figure 1B). However, there was a trend of more dead cells when the MPBs were shipped at 25C. Despite reduced CD45 cells within the MPBs shipped at 25C, the percentages of CD34 cells were similar to percentages noted in MPBs received at 4C (Table 1). A calculation of the total recovered CD34 cells was markedly reduced when the cells were shipped at 25C as compared to shipment in the cold (Table 1). The total number of retrieved cells were 12 10 and 10 10 at 4C and 25C shipment, respectively. When the number of CD45/CD34 cells were calculated, this resulted in 41 10 for 4C shipment and 26 10 for 25C shipment. These results indicated loss of CD34 cells at room temperature shipment, indicating more efficient recovery of total CD34 cells when the MPBs were shipped at 4C.
Table 1 Recovered CD34 cells in MPBs shipped on ice or room temperature
| LeukoPak | Shipping Temperature | Total MNCs | Total CD45/34 Cells |
| 93 mL | 4C | 12 10 | 41 10 |
| 91 mL | 25C | 10 10 | 26 10 |
| One fourth of an MPB sample was shipped in leukopak at 4C or 25C. Immediately after arrival to the laboratory the samples were analyzed for total CD34 hematopoietic cells. | |||
This section studied the outcome of cryopreserved cells that were shipped at 4C and 25C. This question was addressed by determining the maximum number of cells that could be stored in 2 mL cryovials, based on recovered CD34 cells. We used a 1:1 ratio of the leukpak solution within the shipped cells and freezing media containing HSA and DMSO (see materials and method section). We cryopreserved 50 10 and 200 10 cells/vial using the described conditions, and compared with cells cryopreserved in Cryostor solution. We also included cells stored with hyothermasol in which the cells were stored for one week in the refrigerator.
At one week in cryopreservation condition, the cells were thawed and equilibrated in RPMI 1640 at 5 10 cells per mL, as described [6]. We assessed the cells’ health as described for Figure 1B, and determined the percentages CD45/CD34 by flow cytometry. Using the cells in the hypothermosol as a reference, the results indicated that MPBs shipped at 4C and at 50 10 cells per vial were the optimal conditions (Table 2). The data seemed to suggest that the ideal conditions would be cryopreserving with CryoStor and shipment at 25C. However, as shown in Figure 1 and Table 1, there were reduced viable cells when the MPBs were shipped at 25C. Altogether, the information indicated optimal conditions for cost-effective cryopreservation of large number of cells are best with HSA and DMSO at 50 10 cells in 2 mL vials.
Table 2 Cell health and CD34 recovery in cryopreserved vials
| CD45CD34 | ||||||||
| Cells | Shipping | Total Cell Health (%) | CD45/ | Cell Health (%) | ||||
| (10)/Vial | Temp | Live | Injured | Dead | CD34 (%) | Live | Injured | Dead |
| 50 | 4C | 72.3 | 15 | 9.4 | 0.75 | 96.4 | 1.6 | 1.6 |
| 200 | 4C | 50.3 | 33.4 | 11.7 | 0.77 | 94.1 | 4.7 | 1.0 |
| 50 | 25C | 27.7 | 40.6 | 24.8 | 0.65 | 86.0 | 12.4 | 1.2 |
| 200 | 25C | 63.1 | 22.2 | 9.1 | 0.88 | 97.2 | 1.8 | 0.6 |
| Cryostor | ||||||||
| 100 | 4C | 61.3 | 27.9 | 6.0 | 0.86 | 69.4 | 22.5 | 6.7 |
| 100 | 25C | 80.5 | 11.9 | 4.6 | 1.03 | 95.4 | 4.3 | 0.1 |
| Hypothermosol | ||||||||
| 50 | 79.7 | 11.0 | 6.0 | 0.87 | 96.2 | 2.8 | 0.6 | |
| MPBs were cryopreserved at 50 or 200 10 cells in 2 mL vials. After one week, the cells were thawed and then equilibrated as described () in RPMI1640 at 5 10 cells/mL. After this, the cells were assessed for vitality and by flow cytometry for CD45CD34 cells. | ||||||||
The analyses thus far supported optimum cryopreservation at 50 10 cells per vial. We therefore analyzed cryopreserved total nucleated cells and CD34 cells in detailed analyses for cell health. The isolation of CD34 cells from MPBs was previously described [6]. As expected, the short- term storage of cells in the cold with hypothermosol, designated as reference (Ref) in Figure 2 showed sustained viability with minimum injured cells for both total nucleated and CD34 cells (Figure 2). These findings were comparable at cell density of 50 10 cells/vial at 4C but not for cells shipped at 25C (Figure 2). The data confirmed that the lower number of cells stored in one vial resulted in better cell health, providing the cells are shipped on ice.
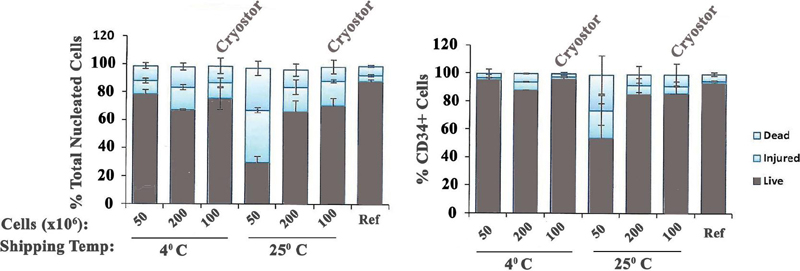
Figure 2 Cell health of CD34 cells in MPBs. Cells shipped at room temperature (25C) and cold (4C) and stored at different concentrations were compared for cell health. The nucleated cells (left) were studied for CD34 cells (right).
Since the shipping and cryopreservation condition affected cell health (Figure 2), we discerned the effects of these conditions on total CD34 cells and subsets (CD38/CD38). Regardless of the condition, the percentages of CD34 cells in the viable CD45 cells were similar (Figure 3A). When the CD34 cells were evaluated based on CD38 expression, the CD34/CD38 subset, which includes hematopoietic stem cells, was similar in all conditions. However, cells shipped at 4C and stored in CryoStor showed the most recovered progenitors/CD34/CD38 (Figure 3B). In total, the shipping and cryopreservation conditions did not alter the percentages of CD34 cells within the MPBs but did alter the progenitor subsets.
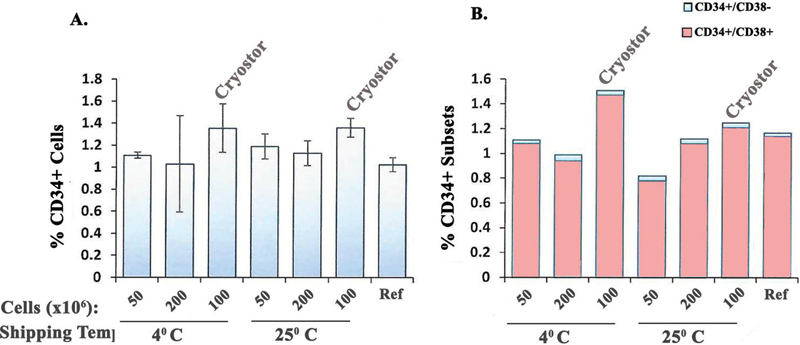
Figure 3 Relative CD34 subset as a function of shipping temperature and cryopreserve cell numbers. A) The different optimized conditions with in-house storage media were compared for total CD34 hematopoietic cells with commercial CryoStor and hypothermosol as a reference (Ref). B) The method in ‘A’ was repeated for CD34 cells expressing CD38.
Thus far, we deduced that the most cost- and resource-effective method to cryopreserve cells was to store at 50 10/vial with MPBs shipped at 4C (Figures 1–3). We therefore thawed vials of stored cells for isolation of CD34 cells with the bead separation method as described [6]. We compared the distribution of CD34 subset within the CD45 population of the thawed cells (Figure 4A) and after selection (Figure 4B). The results showed 18 times enrichment of CD34CD38 cells, which contained the hematopoietic stem cells (Figures 4A and 4B – middle panels). The progenitor cells (CD34CD38) were enriched 40 times (Figures 4A and 4B – middle panels). The viability was similar before and after isolation, based on 7-AAD exclusion (Figures 4A and 4B – right panels). In total, the optimal storing conditions recovered different hematopoietic progenitor subsets.
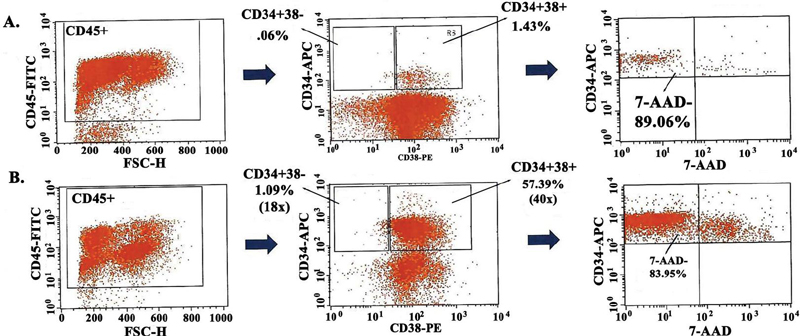
Figure 4 Relative recovery of CD34CD38/ cells from cyropreserved MPBs. A) MPBs were thawed and equilibrated and then analyzed for CD34CD38 and CD34CD38. The cells were studied for viability (right panel), B) The equilibrated MPBs were used to isolate CD34 cells and then analyzed for CD38 expression, and viability.
This section describes if there was below the threshold of contaminating immune cells within the isolated CD34 cells, isolated from crystored cells. We first studied the population of T-cells, B-cells, and myeloid cells after the MPBs were thawed. The results showed significant immune cell recovery (Figure 5A). After isolation of CD34 cells, the presence of T- and B-cells were significantly reduced with almost no NK cells (Figure 5B). These findings indicated that the MPBs stored at optimal conditions could recover CD34 cells that could be used for humanization of immune deficient mice [8].
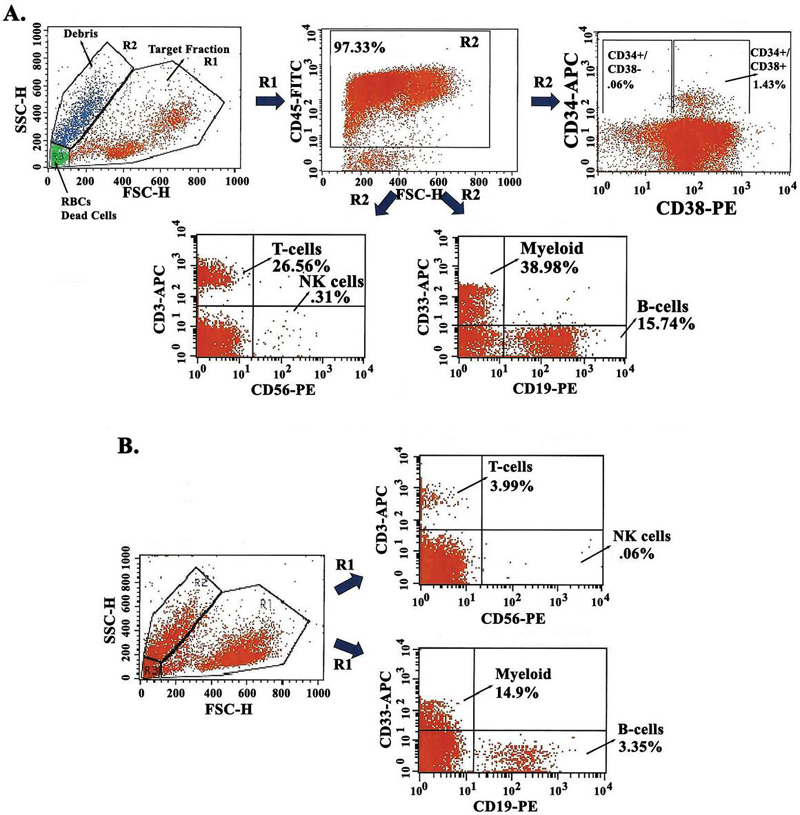
Figure 5 Immune cells in isolated CD34 cells from cryopreserved MPBs. A) MPBs were thawed and equilibrated and then analyzed for different CD34 cell subset, T-cells, B-cells and myeloid cells by flow cytometry. B) The thawed cells were used to isolate CD34 cells and then analyzed for immune cells as described in ‘A’.
This study reports on a cost-effective, yet efficient process to cryopreserve large number of primary cells. The described processes is significant to cells with limited capacity to expand in vitro. Research laboratories, biotechnology companies and start-up research laboratories, in general, have limited resources. These laboratories could apply the described processes to cryopreserve valuable primary cells for long-term studies. The processes described in this study could be important to the costly method to establish immune deficient mice with human hematopoietic system. Due to cost. and perhaps control of the same donor cells in experimental groups, scientists are engaged with in-house humanization of the mice as opposed to mice from commercial sources. A large number of cells are required for these studies, which require the use of MPBs. These cells are expensive to acquire from commercial sources, such as the one described in this study. MPBs could be acquired from the hematopoietic transplant center at any institution. This could be acquired from remaining MPBs after a successful transplant, or if the harvested MPBs are no longer needed because the patient expired. The use of MPBs will require special review and approval by the human subject review committee of the specific institution.
This study compared shipment of the cells at room temperature and on ice, based on cell health and recovered hematopoietic progenitors following cryopreservation. The data indicated efficiency when the cells were shipped on ice. More importantly, cryopreservation of 50 10 cells/vial led to better recovery of hematopoietic progenitors. The low percentages of differentiated immune cells after CD34 isolation indicated that the described method could be sufficient for transplantation of immune deficient mice without evidence of graft versus host response, as previously reported [6]. However, the tolerable amounts of immune cells in the isolated population will have to be determined by the specific experimental question, and the scientific group.
Although this method selected MPBs, other sources of hematopoietic cells can be used to isolate hematopoietic cells. Such sources could be umbilical cord blood and bone marrow aspirate. The total mononuclear cells from these hematopoietic cell sources are expected to be relatively less as compared to MPBs. This will allow for a smaller number of cells to be cryopreserved per vial. In this regard, there will be efficient cell recovery of viable cells.
We performed robust studies that compared two different shipping temperatures. This issue is relevant considering the growing number of commercial sources that provide human samples such as peripheral blood and MPBs. It is important to determine the specific experimental questions when deciding to use a commercial source to acquire human hematopoietic tissues. Perhaps, the experiments might require fresh samples. In this regard, the scientists will need to get the samples at the host institution or at a nearby hospital.
Primary stem cells such as mesenchymal stem cells (MSCs) from different sources such as bone marrow, adipose and placenta do not require large number of cells in one vial [9–11]. However, unlike hematopoietic cells, MSCs are easily expanded, which could allow for early cryostorage of expanded MSCs. These early passaged cells could be stored to ensure continuation of studies that require a large number of cells at an early passage. In summary, this study reports on experimental options when working with primary cells that cannot be expanded. The baseline report can be modified to adapt to the specific experimental questions.
The Bosarge Family Foundation supported this work.
SA performed the experiments and analyzed the data; SSG provided the concept of the studies, and analyzed the data; KG performed the experiments and analyzed the data; LSS wrote the paper and analyzed the data; BS wrote the paper and analyzed the data; AP wrote the paper and analyzed the data; YK wrote the paper and analyzed the data; PR wrote the paper, provide the conceopts and analyzed the data.
[1] Sterner RC, Sterner RM. CAR-T cell therapy: current limitations and potential strategies. Blood Cancer J. 2021;11(4):69.
[2] Wei X, Yang X, Han Z-p, Qu F-f, Shao L, Shi Y-f. Mesenchymal stem cells: a new trend for cell therapy. Acta Pharmacologica Sinica. 2013;34(6):747–54.
[3] Thomas ED. Bone marrow transplantation: a historical review. Medicina. 2000;33(3):209–18.
[4] Dreger P, Haferlach T, Eckstein V, Jacobs S, Suttorp M, Löuffler H, et al. G-CSF-mobilized peripheral blood progenitor cells for allogeneic transplantation: safety, kinetics of mobilization, and composition of the graft. Br J Haematol. 1994;87(3):609–13.
[5] Treleaven JG, Mehta J. Bone marrow and peripheral blood stem cell harvesting. J Hematother. 1992;1(3):215–23.
[6] 6. Greco SJ, Ayer S, Guiro K, Sinha G, Donnelly RJ, El-Far MH, et al. Restoration of aged hematopoietic cells by their young counterparts through instructive microvesicles release. Aging (Albany NY). 2021;13(21):23981–4016.
[7] Bender JG, Unverzagt K, Walker DE, Lee W, Smith S, Williams S, et al. Phenotypic analysis and characterization of CD34 cells from normal human bone marrow, cord blood, peripheral blood, and mobilized peripheral blood from patients undergoing autologous stem cell transplantation. Clin Immunol Immunopathol. 1994;70(1):10–8.
[8] Gergues M, Ayer S, Morelli S, Greco SJ, Rameshwar P. Hematological Humanization of Immune-Deficient Mice. Methods Mol Biol. 2021;2224:195–202.
[9] Romagano MP, Sherman LS, Shadpoor B, El-Far M, Souayah S, Pamarthi SH, et al. Aspirin-Mediated Reset of Preeclamptic Placental Stem Cell Transcriptome – Implication for Stabilized Placental Function. Stem Cell Rev Rep. 2022;18(8):3066–82.
[10] Sherman LS, Condé-Green A, Naaldijk Y, Lee ES, Rameshwar P. An Enzyme-free Method for Isolation and Expansion of Human Adipose-derived Mesenchymal Stem Cells. J Vis Exp. 2019(154).
[11] Sherman LS, Shaker M, Mariotti V, Rameshwar P. Mesenchymal stromal/stem cells in drug therapy: New perspective. Cytotherapy. 2017;19(1):19–27.
International Journal of Translational Science, Vol. 1, 29–42.
doi: 10.13052/ijts2246-8765.2024.002
© 2024 River Publishers